Setup
- Probe: Linear
- Mode: Peds Abdomen
- Depth: 4cm
Views
- Pylorus in short axis
- Pylorus in long axis
- Clip of food passing or unable to pass through pylorus
Scanning
- Place the patient in a supine or R lateral decubitus position.
- Place the probe in the epigastrium with marker facing patient’s right.
- Use the liver and gallbladder as acoustic window to visualize the pylorus in long axis.
- Image channel without moving for a period of time to visualize whether food is passing from stomach to small bowel.
- Turn the probe maker towards the patient’s head to visualize the pylorus in short axis, but pyloric orientation is not the same in every patient.
Normal Measurements
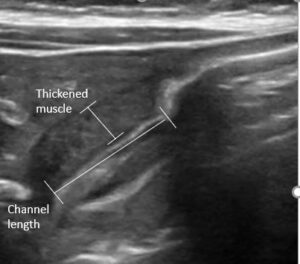
- Channel length < 14 mm
- Muscle wall < 3mm

Pyloric Stenosis in Long Axis
Pyloric Stenosis in Short Axis
![]()
Unable to identify pylorus
Fix → Increase depth to identify landmarks (liver, gallbladder, stomach). Once stomach is identified, decreased depth, and follow stomach antrum to pylorus.
Measurements are incorrect
Fix → Measure only the hypoechoic muscle layer on the near side of channel to probe.
Pylorospasm
Fix → Transient muscle spasm can appear like pyloric stenosis by obstructing flow and thickening muscle. Pylorospasm will resolve with feeding, while pyloric stenosis does not.