Set-up
- Probe: Linear
- Mode: Peds Abdomen
- Starting Depth: 4 cm
Views
- Psoas muscle
- Iliac vessels
- Appendix
- Long axis with blind sac connected to cecum
- Short axis with target sign
Scanning
- Start at point of maximal tenderness
- If appendix not identified, use anatomy to orient and localize ileoceal junction
- Trace cecum to appendix
- Use graded compression to eliminate gas artifact and assess appendix compressibility
Abnormal measurement
- Diameter > 6 mm
Appendix in long axis
Blind ended tubular structure, usually < 6cm in diameter, compressible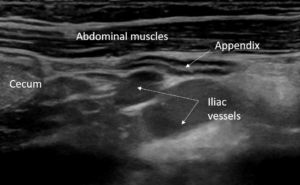
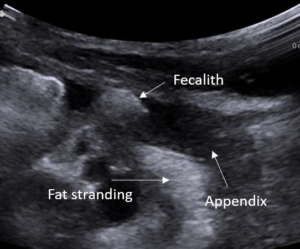
Appendicitis
Appendix is > 6 mm, non-compressible 
Fat Stranding, Fecalith
Secondary signs suggestive of appendicitis
Free Fluid

Appendix obscured by bowel gas
Fix → Move bowel gas out of view using graded compression, or reposition patient
Thickened ileum is mistaken for appendix
Fix → Identify blind ended tip and trace back to cecum
Fix → Visualize entire length of appendix to the blind end of the tip False positive interpretation
Fix → A normal appendix can be > 6mm. For a positive finding, there must be an enlarged, non-compressible appendix + signs of inflammation on ultrasound or lab work, and pain